Mictum Miggo1, Innocent Khuliwa1, Denilson Eugenio1, Mathews Saindi1, Thokozani Nankhonya1, Richard Kamalizeni1, Emma Kamoto 1, Felistus Kazingatchire1, 3, Patience Chikuse1, Hamstone Lwesha4, Johnstone J. Kumwenda2
- St. Joseph’s Mission Hospital –Nguludi, Malawi
- Kamuzu University of Health Sciences, Blantyre, Malawi
- Elizabeth Glaser Pediatric AIDS Foundation, Malawi
- Kamuzu Central Hospital, Lilongwe, Malawi
Corresponding author: Mictum Miggo. E-mail: mictummiggo@live.com
Abstract
A 27 year old man presented with a history of weight loss and generally feeling unwell for more than 2 years. He had several negative HIV rapid tests. His wife had a positive HIV test in 2023 during screening while she was pregnant with their first child. When HIV RNA test was requested, it was positive with a viral load of 1,740, 000 copies/ml. In patients in high HIV prevalence settings suspected to have HIV infection with repeated negative rapid antibody diagnostic tests, HIV RNA testing should be requested to exclude infection.
Key words: Human Immunodeficiency Virus, misdiagnosis, false negative HIV antibody tests
Case Description
A 27 years old man presented to St Joseph Hospital, Malawi with a two-year history of feeling unwell. He complained of abdominal pain, intermittent episodes of loose stools, and intermittent fevers for five-months and weight loss for two years. His wife tested positive for HIV during pregnancy in 2023. His HIV test was negative at that time. These tests were carried out while they were living in South Africa. The wife returned to Malawi immediately after this test. He remained in South Africa until 5 months before presenting to our hospital. He had visited several health centers before coming to our hospital. HIV tests were carried out using antibody rapid tests. These were all reported to be negative. On examination, he was pale, cachectic with a Body Mass Index of 11.5 m2/Kg (see picture with permission from the patient), he had low grade fever of 37.5oC, he had mild abdominal tenderness. He needed support to sit. The rest of the examination was normal. We repeated the HIV rapid test using the Malawi National HIV testing guidelines. The rapid HIV test result came back negative. At this point we reached out to John Hopkins Project laboratory, Blantyre, Malawi for an HIV viral load test. The test came back positive with an HIV viral load of 1,740, 000 copies/ml. His CD4 cell count was 12 cells/mL. At this point, we did a urine Tuberculosis (TB) Lipoarabinomannan (LAM) test and serum Cryptococcal Antigen (CRAG) as recommended by the National Antiretroviral Therapy (ART) Program. His urine LAM was positive, but serum CRAG was negative. We started him on treatment for disseminated TB. The rest of the investigations are shown in the tables below. Unfortunately, the patient died eight days after starting TB treatment.
Investigation and Results
Following laboratory investigations, the following results were obtained:
Table 1: Full blood count report
| Parameter | Result | Reference Unit |
| White cell count | 4.9 | 4.0 -10.0 10^9/L |
| Hemoglobin | 9.1 | 12.0 -16.0 g/dl |
| MCV | 76.2 | 80.0 -100.0 fL |
| Lymphocytes number | 1.0 | 0.8-4.0 10^9/L |
| Red blood cells | 3.63 | 4.0-5.50 10^12/L |
| Granulocytes number | 3.3 | 2.0 -7.0 10^9/L |
| Platelets count | 106 | 150 -450 10^9/L |
Table 2: Liver function test
| Parameter | Result | Reference Unit |
| SGOT | 44 | up to 46 U/L |
| SGPT | 27 | up to 49 U/L |
| Direct Bilirubin | 0.26 | up to 0.4 mg/dl |
| Total Bilirubin | 0.32 | 0.1-1.2 mg/dl |
| Alkaline phosphate | 81 | 80-306 U/L |
| Albumin | 31.8 | 35-55 mg/dl |
| Total protein | 56.4 | 62-80 mg/dl |
| GGT | 21.4 | 5-32 U/L |
| LDH | 380.3 | 225-450 U/L |
Table 3: Urine dipstick results
| Parameter | Result |
| Color | Amber |
| Appearance | Hazy |
| Protein | +1 |
| Glucose | Negative |
| Ketones | Negative |
| Specific gravity | 1.025 |
| Ascorbic acid | Negative |
| Leucocytes esterase | Trace |
| Nitrites | Negative |
| Blood | + |
| PH | 6.5 |
| Urobilinogen | Negative |
| Bilirubin | Negative |
| White blood cells | Negative |
| Red blood cells | Negative |

Figure 1: Patient picture

Figure 2: Patient picture
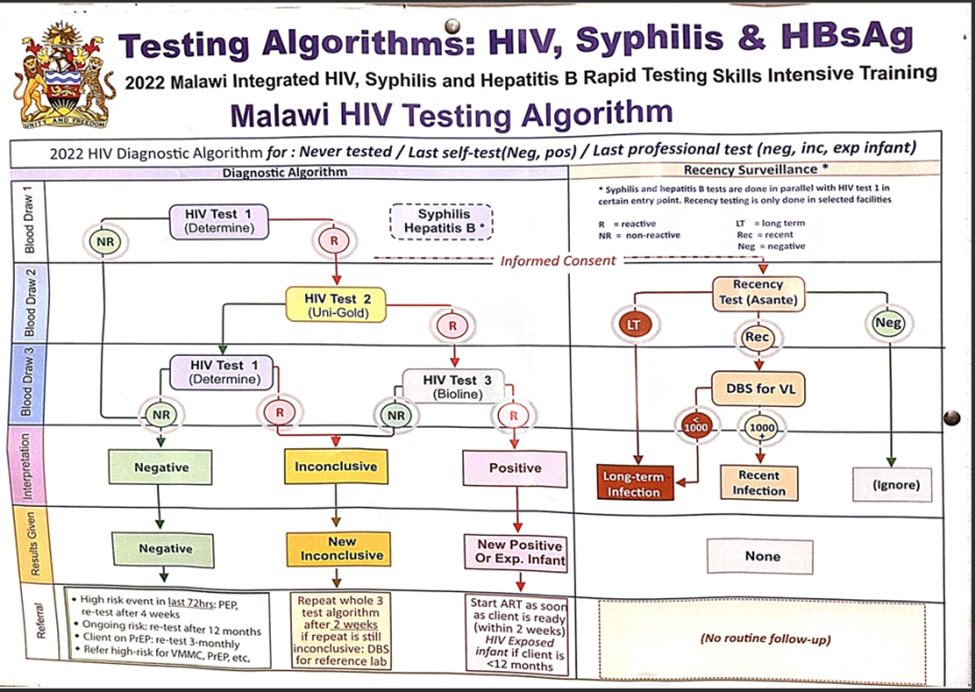
Figure 3: HIV, Syphilis and Hepatitis B testing pathway
Discussion
Seronegative HIV infection using the current testing pathways is a very rare phenomenon. A meta-analysis of 64 publications on the subject found a small proportion of false negative (median: 0.4%, interquartile range (IQR); 0-3.9%); diagnoses were identified 1. In this study suboptimal testing strategies were the most common factor in studies reporting misdiagnoses. A substantial proportion of false negative diagnoses were related to retesting among people on antiretroviral therapy. Several cases have been reported especially from sub-Saharan Africa about this phenomenon. The case reports both from Tanzania have reported separate cases of Advanced HIV Disease (AHD) having repeatedly tested HIV negative using the rapid test pathway2, 3.
Our patient was not on ART. He was tested in several facilities both in Malawi and Republic of South Africa. In our view, he was true false positive. It is inconceivable that all the facilities that tested him used suboptimal testing strategies. Other reasons must explain this. Did he have a genetically diverse virus that could not be picked by the usual tests? A case report from Botswana may mirror our patient. A case of antibody-negative human immunodeficiency virus type 1 (HIV-1) subtype C infection has been reported. The case was identified using HIV RNA during a study of acute HIV infection4. Results of tests for HIV-1 antibodies were consistently negative, including rapid and regular enzyme-linked immunosorbent assay and Western blot. The non-recombinant HIV-1 subtype C infection was confirmed by viral genotyping within the gag, pol, and env genes4, 5, 6.
Lessons learned
Current HIV rapid diagnostic tests are very sensitive. A false negative antibody test for HIV after a window period is very rare. However, in areas with a generalized epidemic and a large prevalence of HIV, such diagnostic dilemmas are likely to occur more frequently7 therefore, the HIV test results need to be interpreted within the context of the patient. Our patient clearly had WHO HIV clinical stage four diseaseand yet the screening tools consistently produced negative test results 8, 9, 10,
This case has taught us that negative rapid HIV test results can occur even in patients with a high suspicion of severe HIV disease. Therefore, the guidelines should consider revising the testing algorithm to allow the addition of an antigen test for HIV diagnosis. The current 4th generation diagnostic test include the P24 antigen which enables earlier identification of HIV infection 11. If these newer tests were included in the diagnostic pathway, our patient’s HIV status would have been identified sooner.
Ethics and consent
The patient and the guardian had consented to participate in the study and consented to pictures used in this report before the patient died
Funding source
This research did not receive any specific grant from funding agencies in the public, commercial or non-profit organizations.
Competing Interests
The authors declare no conflicts of interest
Acknowledgements
We acknowledge the medical team at St Joseph’s Mission Hospital-Nguludi who took care of this case. We thank the Johns Hopkins Project Laboratory.
References
- Johnson CC, Fonner V, Sands A, Ford N, Obermeyer CM, Tsui S, Wong V, Baggaley R. To err is human, to correct is public health: a systematic review examining poor quality testing and misdiagnosis of HIV status. Journal of the International AIDS Society. 2017 Aug;20:21755.
- Chuwa F, Kivuma B, Ndege R, KIULARCO Study Group. Repeated false-negative HIV rapid test results in a patient presenting to care with advanced HIV disease: A case report. IDCases. 2023 Jan 1; 31:e01719.
- Ibrahim PM, Haddadi S, Luhuti K, Illonga Z, Kasyanju L, Mkinde Z, Mwandigha A, Magorosa E, Mushi B, Ngaiza A, Mmbaga E. Dilemmas in diagnosing advanced HIV disease: a case report of repeatedly false negative rapid HIV tests in a patient with epidemic Kaposi sarcoma in Tanzania. Critical Public Health. 2025 Dec 31;35(1):2499127.
- Novitsky, V., Gaolathe, T., Woldegabriel, E., Makhema, J. and Essex, M., 2007. A seronegative case of HIV-1 subtype C infection in Botswana. Clinical Infectious Diseases, 45(5), pp.e68-e71.
- Brown P, Merline JR, Levine D, Minces LR. Repeatedly false-negative rapid HIV test results in a patient with undiagnosed advanced AIDS. Annals of internal medicine. 2008 Jul 1;149(1):71-2.
- Kufa T, Kharsany AB, Cawood C, Khanyile D, Lewis L, Grobler A, Chipeta Z, Bere A, Glenshaw M, Puren A. Misdiagnosis of HIV infection during a South African community‐based survey: implications for rapid HIV testing. Journal of the International AIDS Society. 2017 Aug;20:21753.
- Khan S, Mafara E, Pasipamire M, Spiegelman D, Mazibuko S, Ntshalintshali N, Hettema A, Lejeune C, Walsh F, Okello V. Identification of misdiagnosed HIV clients in an Early Access to ART for All implementation study in Swaziland. Journal of the International AIDS Society. 2017 Aug;20:21756.
- Malawi Integrated Clinical HIV Guidelines 5th Edition (2022); https://dms.hiv.health.gov.mw/dataset/malawi-intergrated-clinicacounsel-hiv-guidelines-1st-edition-2022: accessed on 24th July,2025, 11:30hrs
- Baylor Tingathe Community Outreach Programme; HIV Diagnostic Assistant Manual. 3rd Edition. 2016; https://www.tingathe.org › hda_participants_manual: accessed on 30th July, 2025 , 23:43hrs
- Obeagu EI, Amaeze AA, Ogbu IS, Obeagu GU. B Cell Deficiency and Implications in HIV Pathogenesis: Unraveling the Complex Interplay. Elite Journal of Nursing and Health Science. 2024;2(2):33-46.
- Lang R, Charlton C, Beckthold B, Kadivar K, Lavoie S, Caswell D, Levett PN, Horsman GB, Kim J, Gill MJ. HIV misdiagnosis: A root cause analysis leading to improvements in HIV diagnosis and patient care. Journal of Clinical Virology. 2017 Nov 1;96:84-8.
